The Problem
Brain injuries are caused by a blow to the head (i.e. due to sports, vehicular accidents, etc.) that results in trauma to the brain. They are extremely common but widely under-diagnosed, unrecognized, and under-supported. In 2013, there were 2.8 million brain injury related emergency department visits, hospitalizations, and deaths across the U.S, and a shocking 42% of people with brain injuries are unemployed while 61% develop depression. Every brain injury is unique, and there is not nearly enough support for those with brain injury.
Synapse National
Synapse is a national nonprofit organization dedicated to combating the isolation individuals with brain injury often face through the creation of a powerful social support network. Originally started at MIT and Stanford, Synapse now has 11 chapters at universities across the united states led by undergraduate students, and 5 more new chapters were recently founded this year.
Learn more at: https://synapsenational.org/
Learn more at: https://synapsenational.org/
Our Chapter's Core Values
Building Community. Being part of a community means standing together, understanding one another, and providing support for one another. This is key to not only recovery but making sure that people with brain injury understand that they are not alone as they go experience their injury. We care.
Integrating Resources. There are plenty of resources in the Seattle area, but these resources need to be centralized. We want to integrate resources and bring it all together in a one-stop-shop for people with brain injury and their families to get the best care for them.
Educating and Raising Awareness. Although brain injury is very common, we need much more awareness about what it is, how to prevent it, and what to do when someone has a brain injury. As such, we want to educate and raise awareness as a first step towards better treatment for brain injuries.
Integrating Resources. There are plenty of resources in the Seattle area, but these resources need to be centralized. We want to integrate resources and bring it all together in a one-stop-shop for people with brain injury and their families to get the best care for them.
Educating and Raising Awareness. Although brain injury is very common, we need much more awareness about what it is, how to prevent it, and what to do when someone has a brain injury. As such, we want to educate and raise awareness as a first step towards better treatment for brain injuries.
What We Offer
All our events are open to all individuals in the community, whether you are a returning member or new to our group! Student meetings are designed to educate our undergraduate members, but any community member who is interested may attend. There is no mandatory RSVP unless specified (e.g. for some of our special outings), but we always appreciate you letting us know you'll be attending by emailing [email protected]. Please see the events page for all event times and locations. You can find applications to the Buddy Program on our Get Involved page.
Peer Support Groups
Peer Support Groups
- Every other week, Synapse hosts Peer Support Groups, where student members come together with brain injury community members to discuss themes surrounding brain injury.
- These events serve as a therapeutic option for our brain injury members to discuss day-to-day challenges and successes.
- Twice per quarter, Synapse hosts themed social events which provide a casual environment where our student and brain injury members can interact.
- Previous social events include trips to the zoo, pets and pals in the Quad, picnic at Gas Works park, Valentine's Day Social, Halloween social, and Potted Plans and Painting.
- The Buddy Program pairs brain injury members with an undergraduate student.
- This program facilitates meaningful 1-on-1 friendships and social relationships, and allows brain injury members to meet some amazing people!
- Twice per quarter, Synapse hosts student-only meetings
- Topics for these meetings include:
- Trainings developed by healthcare professionals and local brain injury related nonprofit leaders on working with individuals with brain injuries
- Review of current brain injury related neuroscience research
- Brain Trivia games
More About Brain Injuries and Synapse
Synapse at the UW is a brain injury support organization. Acquired brain injury describes any damage to the brain sustained after birth. This is in contrast, for instance, to brain injuries acquired while in the womb or due to fetal alcohol syndrome.
ABI is then broadly divided into two categories: Traumatic Brain Injury (TBI) and Non-Traumatic Brain Injury. “Trauma” here is not in reference to the severity, seriousness, or emotional impact of the injury. Rather, “trauma” refers physical, external damage. In the case of TBI, a TBI is defined as a “external strike or blow to the head causing injury,” such as a heavy object falling on one’s head, domestic abuse, etc. In contrast, a non-TBI often often refers to damage occurring internally. Examples of non-TBI include stroke, hypoxia, and substance abuse. Stroke tends to be the most common non-TBI, where blood flow to the brain is restricted, thus resulting in cellular damage/death. Notice how this injury is “internal” or involves internal processes/damage whereas TBI involves some external force impinging on the head.
Synapse at the UW is technically an ABI-support organization. Many of our clients have experienced stroke. However, we continue to refer to ourselves as a TBI support organization because this is what the national organization refers to itself as. We welcome all people with ABI, both traumatic and non-traumatic. We do not discriminate or turn away based on this medical dichotomy!
ABI is then broadly divided into two categories: Traumatic Brain Injury (TBI) and Non-Traumatic Brain Injury. “Trauma” here is not in reference to the severity, seriousness, or emotional impact of the injury. Rather, “trauma” refers physical, external damage. In the case of TBI, a TBI is defined as a “external strike or blow to the head causing injury,” such as a heavy object falling on one’s head, domestic abuse, etc. In contrast, a non-TBI often often refers to damage occurring internally. Examples of non-TBI include stroke, hypoxia, and substance abuse. Stroke tends to be the most common non-TBI, where blood flow to the brain is restricted, thus resulting in cellular damage/death. Notice how this injury is “internal” or involves internal processes/damage whereas TBI involves some external force impinging on the head.
Synapse at the UW is technically an ABI-support organization. Many of our clients have experienced stroke. However, we continue to refer to ourselves as a TBI support organization because this is what the national organization refers to itself as. We welcome all people with ABI, both traumatic and non-traumatic. We do not discriminate or turn away based on this medical dichotomy!
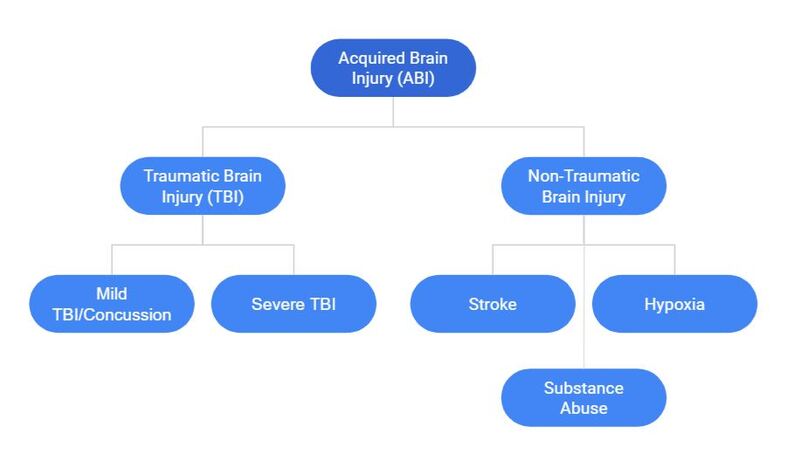
What’s more, TBI is often divided into two categories. Division of people into these categories can be intensive and, at times, subjective. The first category of TBI is “Severe TBI.” Severe TBI has a loose definition, and diagnosis is often an amalgam of clinical considerations. For instance, most patients who stay in the hospital for extended periods of time or who experience a coma are often considered severe cases. Attempts at quantitative evaluations of TBI have also been made, including the famous assessment tool of TBI: the Glasgow Coma Scale. Essentially, upon admittance to the emergency dept., clinicians will perform this test to assess how severe one’s injury is. Scores of 8 or less indicate a severe TBI. One will immediately notice, however, that these measures are all extremely subjective, making diagnosis/treatment difficult, especially during the acute phase of the injury.
In contrast, the other category of TBI is “Mild TBI” also known more colloquially as “Concussion.” Clinicians tend to prefer the term “concussion” because it sounds less-bad than a “mild TBI.” A few studies have even shown that referring to the injury as a “concussion” vs. “mild TBI” has a correlation with improved patient outcomes, purely based on perception of injury. Most of the clients we serve will have experienced mild TBI. Mild TBI is associated with a higher Glasgow Coma Scale score, and patients often do not undergo as intensive of care. Indeed, whereas severe TBI may include the consult of neurosurgeons. Neurologists, vision specialists, and others, people with TBI are often told to rest and have much less demand on ‘follow-up appointments.’
It is important to remember that both mild and severe TBI have diverse symptoms that can be a huge bearing on one’s life. Symptoms can last weeks to months to even years. Just imagine: your brain can be damaged in so many different ways during a car accident or if something falls on your head. As such, everyone’s experience with TBI is unique, and “mild” TBI does not mean dismissible! (Really, we exist as an organization in part because support for these populations is lacking!)
There is a large variance in symptom severity and onset times - there is no “one-size-fits-all,” “right” answer to what the effects of brain injury are. Common symptoms include ones that are physical (e.g. light sensitivity, fatigue, paralysis, speech impediments), neurological (e.g. confusion, disorientation, slowed learning, memory loss), and emotional/social (e.g. loss of social barriers, agitation, anxiety).
In contrast, the other category of TBI is “Mild TBI” also known more colloquially as “Concussion.” Clinicians tend to prefer the term “concussion” because it sounds less-bad than a “mild TBI.” A few studies have even shown that referring to the injury as a “concussion” vs. “mild TBI” has a correlation with improved patient outcomes, purely based on perception of injury. Most of the clients we serve will have experienced mild TBI. Mild TBI is associated with a higher Glasgow Coma Scale score, and patients often do not undergo as intensive of care. Indeed, whereas severe TBI may include the consult of neurosurgeons. Neurologists, vision specialists, and others, people with TBI are often told to rest and have much less demand on ‘follow-up appointments.’
It is important to remember that both mild and severe TBI have diverse symptoms that can be a huge bearing on one’s life. Symptoms can last weeks to months to even years. Just imagine: your brain can be damaged in so many different ways during a car accident or if something falls on your head. As such, everyone’s experience with TBI is unique, and “mild” TBI does not mean dismissible! (Really, we exist as an organization in part because support for these populations is lacking!)
There is a large variance in symptom severity and onset times - there is no “one-size-fits-all,” “right” answer to what the effects of brain injury are. Common symptoms include ones that are physical (e.g. light sensitivity, fatigue, paralysis, speech impediments), neurological (e.g. confusion, disorientation, slowed learning, memory loss), and emotional/social (e.g. loss of social barriers, agitation, anxiety).
